The ICE… is gonna BREAK!

“He who cannot put his thoughts on ice should not enter into the heat of dispute.”
― Friedrich Nietzsche, Human, All Too Human

The ultimate temperature test of a Police Pension Authority’s malevolence towards injury awards is how they consider what is a self-created paradox of the ‘band one issue’.
The end game of some Police Pension Authorities is to achieve reduction of all injury pension payments by means of unlawful reviews. But what to do with those who can’t be reduced further? What to do with disabled former officers who are on band one, the lowest band of payment?
Band one presents them with a conundrum. Their thoughts run like this. Reviewing band one pensions might open a box of worms. Should we review them? If we do, then we can’t reduce them, so it would be a waste of time and money, but some of them might well qualify for an increase in payment, which would cost us money. We might also uncover a lot of historical maladministration and face endless complaints, appeals and litigation, which would also cost us money. If we don’t review them, then we leave ourselves open to accusations of disablement discrimination. We can hardly claim we have a duty to review if we then decide not to review band ones.
For so long as these rogue police pension authorities try to justify the contradiction that it’s ‘not all about savings’ whilst holding reviews which so very obviously are for the sole purpose of attempting to save money, they will find it harder to maintain their stance indefinitely and, meanwhile the ice they skate on is getting thinner and thinner.
Staffordshire Police, for example, have a tendency to use dubious practices when an injury award is first decided, such as using their arcane Police Earning Assessment Matrix, to bias the calculation of the degree of disablement heavily so as to only produce disablement levels within band one.
Other police forces such as Merseyside and Nottinghamshire go out of their way to review those in receipt of a band two award and above, so regularly and unlawfully that it just becomes a matter of time until the medical retirement officer civilian or the ‘gun for hire’ SMP succeeds in reducing the award to levels acceptable to the force accountants, but unacceptable and unlawful in respect to legislation.
Merseyside clearly implied in their answer to a freedom of information request that people with injury awards can only ever improve, never deteriorate. In any case, it seems Merseyside is of the opinion that if the people they medically retire do deteriorate they can’t be bothered to find out. Action by a public authority cannot be lawful unless there is a positive power that falls within legal restrictions and discharges lawful duties. Cherry-picking how and when to impose a power isn’t any of these things.
Band 1 will not be reviewed unless requested by the former officer and in that case they would be seen as a priority.
“Seen as a priority” can be interpreted as getting a quick phone call back from Merseyside, from a panicky medical retirement officer, who is intent on convincing the vulnerable that it’s futile to attempt to justify an increase to an award.
Then there are forces like Cambridgeshire, who zealously carried out the unlawful Home Circular 46/2004 whilst deceitfully telling those it affected that it was never about the money, when, in reality, it was always all about the money. Cambridgeshire spent a small fortune of taxpayers’ money in pursuit of illusive savings only to find they were on a fool’s errand. In 2010, Cambridgeshire suspended all reviews. Then in 2012 produced a new policy which limited the number of reviews. Recently there has been a decision to suspend their so-called ‘proactive’ review program. A report to Cambridgeshire Constabulary’s Force Executive Board by the new Director of Human Resources, who runs the recently-formed tripartite Beds/Cambs/Herts HR function, recommends,
‘That in the absence of current national guidance on Injury Award Reviews and the diminishing likelihood of accruing further savings, the current proactive review process be suspended. Recipients will still be able to request reviews where, for example, they believe that there has been a significant change in their degree of disablement, relative to the relevant injury.’
And –
‘The process of carrying out first reviews has generated some savings through the reduction in bandings of allowance for some recipients. However, experience shows that any further reductions in bandings is less likely as a result of second and further reviews.’
Ooops! A bit of a slip there. Do we hear the ominous crack of breaking ice? An admission by Cambs that the driving force behind reviews has always been to achieve savings. No mention of the true intent of the provision of a review process in the Regulations, which is to ensure that disabled former officers continue to receive the amount of injury pension which their disablement qualifies them for, should their degree of disablement alter substantially – for worse, or for better. We suspect, however, that it is less of a slip but rather some sure-footed footwork by a Director who has her heart and her brain fully ethically engaged. She has perhaps recognised the dreadful impact which unlawful or unnecessary reviews bring, to the individuals concerned, and in a different, financial, budget-busting way, to the forces concerned.
The review provision in the Regulations care not what band a person is. The Regulations are blind to the cost implications. Approaching reviews from the point of view of using them to save money is unlawful and immoral. As we have said many a time, injury awards are a form of compensation of work related injuries quantified by the affect the injury has had on a person’s capacity to earn.
Instead of their true purpose, some police pension authorities have corrupted injury awards into the politics of welfare, to what can be termed a ‘race to the bottom’; that is, a drive to cut costs, provision and standards.
There would be a massive improvement in the discourse of injury awards if those who administer the Regulations would calm down enough to think hard about what was being said and to examine its possible truth value.
If the rogue Police Pension Authorities could, for once, examine the ‘heat’ they put into liking or advocating the unpleasant things, plastered all in the emails they distribute between themselves behind closed doors, and start to see the light, there would less opportunity for any independent observer to incessantly impute badness to these people.
Their public face says reviews are nothing to do with the money. Safely sat at their desks their half-truths and lies are forgotten whilst the hot potato of unlawful reviews is put aside to allow them to concentrate on the pressure from above, from the bean-counters and ignorant Chief Constables who see only balance sheets.
The burning – indeed ice melting – question is why would a certain HR manager, one who has been at the centre of the review fiasco in Avon & Somerset since its inception, think its appropriate to ask her force’s Finance Director whether band ones should be reviewed?
There’s nothing in the Regulations to say band ones should be treated any differently from any other band … so, with asinine brashness, Avon & Somerset’s Police Human Resources Manager of Planning, Christine Jones, brings the whole massive iceberg to the surface in her witless puzzlement of why the heck are they even considering to review band ones!
Come on guys, what’s the point? – she asks. It’s not as if we can reduce them any further!

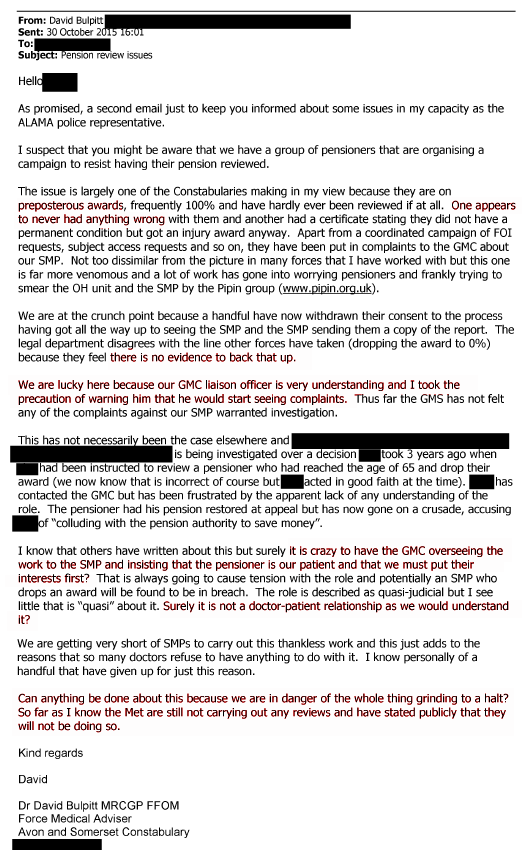
Realising the thin ice that Jones is blundering across has not only cracked but in danger of shattering, Dr Bulpitt, the force’s highly paid Medical Advisor, attempts damage limitation concerning any ‘wild’ assertion from his staff that this is all about reducing people and saving money.
With a rheumy eye to future disclosure under the Freedom of Information Act, Dr Bulpitt, steps in to suggest that he is only doing this mass review program for the benefit of the unfortunate band ones!

So, according to the kindly, caring Dr David Bulpitt, those former officers who are on the highest band, classified in the Regulations as being the victims of ‘very serious disablement’ as a result of performing their duty, are nothing less than ‘selfish’ and ‘fortunate’.
It seems, from this memo, that once Bulpitt thinks the cracking, popping, chirping and pinging from the ice has lessened from Jones’ heavy footfalls, his Tourettes kicks in and normal service resumes. He reverts to his usual nasty, brash, inconsiderate, disability discriminatory self. His memo reveals he thinks his attempts to say as many people should be increased than reduced has stopped the ice from weakening.
His disingenuous claim that reviews are ‘all about the band ones‘ doesn’t, in any way imaginable, mask his claim that those forced to end their career with a severe disability to their earning capacity are ‘fortunate‘ and ‘selfish‘ in their desire to be treated both with dignity and within the law.
Let’s be clear – a doctor, a highly paid medical professional, employed by a police force, has gone on public record that people with a severe degree of disablement which ended their police career are ‘fortunate’ and ‘selfish’.
Why is Dr Bulpitt’s statement about band ones all pretence and covering-his-back bluster? Because in Avon & Somerset between 2005 to 2010 there was not a single increase to any injury award at all. Not only was no single person with a band one increased, there were no increases at all of any banding.
Dr Bulpitt could, of course, send a letter out to every one of the 70 band ones identified by Christine Jones and ask them politely if there has been a deterioration to their medical condition. It is fair to say the probability of him sending such a letter is less than that of Donald Trump converting to Islam and still being elected President.
Dr Bullpitt could also, of course, recommend to his Police Pension Authority, who is the Chief Constable, that he hire another SMP just to review all those on band one. Band one pensioners would be unlikely to object, wouldn’t they? He has chosen not to make that recommendation, for the simple reason that his words are a sham. He has no intention of wanting to see band ones reviewed. He records his fake concern for them only to lay down a get out of goal free card, should he need it. Perhaps this is a sign that he realises the end is now not very far away?
Just like the dungeon scene in Monty Python’s Life of Brian, Dr Bulpitt is effectively saying this to those on any award higher than a band one: You lucky, lucky bastards. Proper little jailer’s pet, aren’t we? You must have slipped the original SMP a few shekels, eh?
There is no sign from this doctor of any understanding that those on higher awards could have been retired with a higher degree of disability simply because their disablement qualified them for it. He seems to be fixate on some unstated conviction that all bands above band one were the result of some sort of ‘fix’. He pays only lip-service to the fact that there are band ones with an award too low for the disability inflicted upon them. It is abhorrent that a clinician, with such callous condescension, can dismiss all historical awards which were given by his predecessors.
The fact is, Dr Bulpitt, that pensioners themselves were not responsible for deciding what band they were awarded. Those decisions were made by senior people within the organisation, overseen by the then Police Authority. Most, probably all of those disabled officers had no knowledge of the Regulations, and in the midst of the trauma of injury and enforced retirement could hardly have been in any fit state to query the decisions of those in authority. If you think that the ‘wrong’ bandings were decided, then why are you calling pensioners selfish and fortunate? Why are you not calling for your predecessors and for former Police Authorities and former Chief Constables to be investigated and made to account for their decisions?
Bear in mind though that those decisions can not now be overturned. The law is very clear on that point. Decisions are final, subject only to appeal within certain time limits, now long past. Also, can you imagine the disastrous publicity which would ensue should any force attempt to hound disabled people, not for mistakes made by them, but for mistakes made by their former force? What would the Home Office have to say about that, Bulpitt? Given that the Home Office might well have been encouraging Chief Officers to rid themselves of disabled officers at that time? A word of advice, Doc – don’t go looking for any support in that direction. They have long decided they want nothing more to do with existing injury pensions; having sipped from the poisoned chalice once they are not coming back for another quaff. Ask the suddenly retired, aged 54, former Chief Constable of Cambridgeshire what support she got from the Home Office when her particular injury pension scam was revealed in all its sordid glory.
We’ve mentioned that Dr Bulpitt seems to be clumsily mitigating Christine Jones’ attitude to band ones, knowing full well that the emails he types can find their way in the public domain. But isn’t it more than likely that Jones is just saying exactly what she has learnt from the jerky personality of Dr Bulpitt? Hierarchy works like this: when anger and intimidation flow down, initiative stops flowing up.
Christine Jones has summarised the whole attitude in Avon & Somerset: Why review when they can’t be reduced further …
And why is this disclosure important?
Because serving officers are currently in the ‘care’ of Dr Bulpitt and the culture of disrespect towards disabled former officer is not confined to them – it extends to any serving officer unfortunate enough to become injured on duty. Dr Bulpitt’s words are but a visible symptom of a deeply-engrained institutional attitude of disrespect which, if allowed to continue uncorrected will have adverse effect on the efficiency and morale of the force.
The link between harsh words and medical errors was reignited in 2012 when Lucian Leape, Professor of Health Policy at the Harvard School of Public Health, published a two-part series in Academic Medicine. Leape and his co-authors asserted that,
‘A substantial barrier to progress in patient safety is a dysfunctional culture rooted in widespread disrespect.’
The series also reported,
‘Disrespect is a threat to patient safety because it inhibits collegiality and co-operation essential to teamwork, cuts off communication, undermines morale, and inhibits compliance with and implementation of new practices.’
The £159,000 remuneration of A&S’s Force Medical Advisor should dictate that the recipient of the salary is beyond reproach in their maintaining of high standards. Sadly the Bulpitt exception proves the rule. Also sadly, it is doubtful whether the Constabulary will do the right thing and dispense with the services of the dubious Dr Bulpitt. They could get a decent doctor for half the price: that’s a legitimate way to save money.
What is certain is that until the culture changes, the maladministration will continue, and people like Dr Bulpitt and Jones and Kern will continue to skate on thin ice until they and this particular police force sinks under the weight of more and more scandals.







Latest Blog Comments